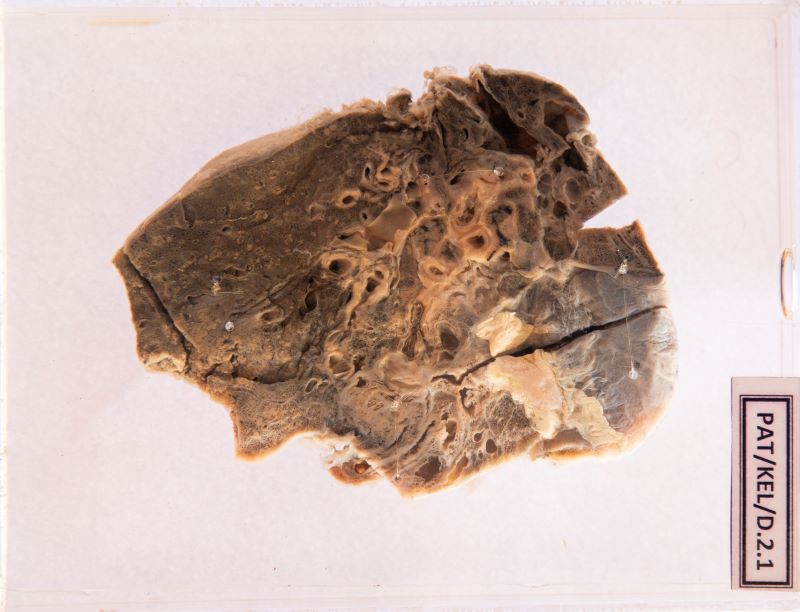
D.2.1 Bronchiectasis with cavitations
- The cut surface shows patchy consolidation towards the apex and confluent grey area in the mid zone.
- The mid zone shows an irregular large cavity made up of confluence of dilated bronchi.
- The walls of the smaller airways are also thickened and plugged with grey material. (Probably pus)

Side 1
Side 2
Clinical presentation
The specimen above shows the lung of a 72 year old woman who died of respiratory failure.
She had a chronic productive cough with copious, foul-smelling sputum and on-and-off haemoptysis for the past 3 years. Gradually she developed shortness of breath.
During the postmortem examination, she was emaciated and had finger clubbing.
Macroscopic appearance
1. Describe the macroscopic changes you observe in this lung specimen.
- Cystically dilated bronchi and bronchioles with thickened walls extending up to the pleura.
- The peribronchiolar lung parenchyma appear pale and consolidated (see image below)
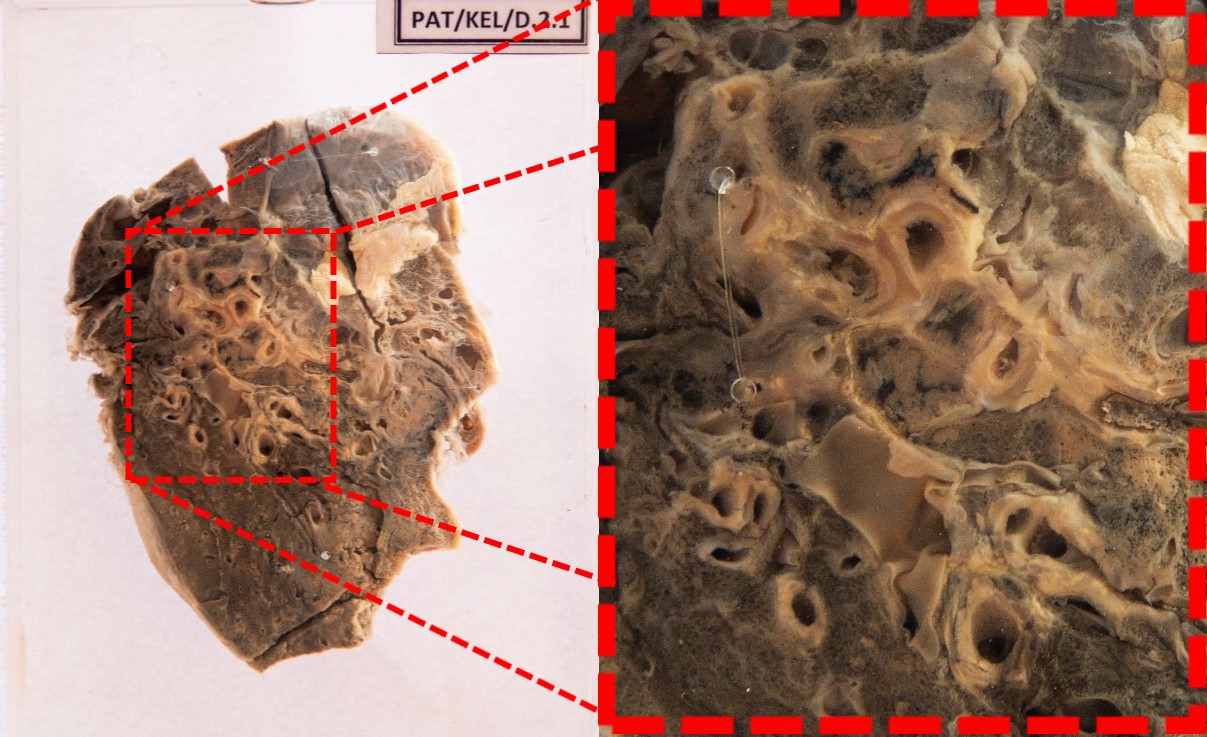
Image - Enlarged appearance of the peribronchiolar lung parenchyma
2. What is the most likely diagnosis?
Bronchiectasis
Microscopic appearance
Describe the microscopic changes you expect to see in the sections taken from the affected areas.
- The walls of the bronchi and bronchioles and the adjacent lung tissue show necrotizing inflammation with luminal obstruction and desquamated lining epithelium.
- Epithelium may show squamous cell metaplasia.
- Abscess formation may be seen seen in the lung tissue.
- Fibrosis of bronchi and bronchioles with luminal obstruction
- Peribronchiolar fibrosis with destruction of normal lung tissue
Pathological basis for the changes
1. Describe the pathological basis for the lung changes you observe.
- Bronchiectasis is caused by various congenital/hereditary conditions, localized or diffuse bronchial obstruction or infective causes.
- Impaired normal mucus clearing mechanisms/ collection of secretions within the bronchi/bronchioles distal to an obstruction increases the susceptibility to infection.
- The infection leads to inflammation and necrosis, damaging the walls of the airways.
- There is destruction of smooth muscle and elastic fibres and fibrosis, leading to permanent dilatation of bronchi and bronchioles